
Intranasal Vaccines: A Potential Off-Ramp For Coronavirus Pandemics
An interesting and also annoying aspect about the human immune system is that it is not a neat, centralized system where you input an antigen pattern in one spot and suddenly every T and B lymphocyte in the body knows how to target an intruder. Generally, immunity stays confined to specific areas, such as the vascular and lymph system, as well as the intestinal and mucosal (nasal) parts of the body.
The result of this is that specific types of vaccines have a different effect, as is demonstrated quite succinctly with the polio vaccines. The main difference between the oral polio vaccine (OPV) and inactivated vaccine (injected polio vaccine, or IPV) is that the former uses a weakened virus that induces strong immunity in the intestines, something that the latter does not. The effect of this is that while both protect the individual, it does not affect the fecal-oral infection route of the polio virus and thus the community spread.
The best outcome for a vaccine is when it both protects the individual, while also preventing further infections as part of so-called sterilizing immunity. This latter property is what makes the OPV vaccine so attractive, as it prevents community spread, while IPV is sufficient later on, as part of routine vaccinations. The decision to use a vaccine like the OPV versus the IPV is one of the ways doctors can tune a population’s protection against a disease.
This is where the current batch of commonly used SARS-CoV-2 vaccines are showing a major issue, as they do not provide significant immunity in the nasal passage’s mucosal tissues, even though this is where the virus initially infects a host, as well as where it replicates and infects others from. Here intranasal vaccines may achieve what OPV did for polio.
Going For The Gut Punch
Logically, targeting intranasal (IN) vaccines to address a coronavirus makes a lot of sense, since coronaviruses are among a group of viruses implicated in e.g. the common cold. Like rhino- and adenoviruses, they are viruses which are strongly adapted to the respiratory system, much like how the polio virus prefers the intestinal tract. Because of this knowledge, multiple intranasal vaccines have been developed and approved, most recently in India and China.
The Chinese vaccine is developed by CanSino Biologics, and it is essentially the same as the regular viral vector-based intramuscular (IM) vaccine, except in a form that allows it to be inhaled in a nebulizer. It is approved for use as a booster after a primary IM-based vaccination course.
The Indian vaccine (BBV154), produced by Bharat Biotech, is intended as a two-dose IN vaccination, rather than only as a booster. Both the CanSino and Bharat vaccines are based on a non-replicating adenovirus vector, which means that no special vaccine formulation is needed for the nebulized form. Upon inhalation of the nebulized vaccine, the adenovirus vector will simply do what it naturally does: get into mucosal cells to deposit its genetic payload.
These IN vaccines join the Iranian Razi Cov Pars vaccine (three-dose recombinant protein subunit-based with IN booster), which received emergency use authorization in Iran on October 31st of 2021. While large-scale efficacy data is not available yet for any of these vaccines, a recent US study in mice has confirmed that a viral vector-based vaccine can induce robust immunity. In a 2021 study by Van Doremalen et al. using the ChAdOx1 nCoV-19/AZD1222 (AstraZeneca) viral vector it was found that IN vaccination of hamsters and macaques prevented large-scale infection and significantly reduced the mucosal viral load.
These findings are essentially why scientists in the West are pushing for IN vaccines to be made available, with some US scientists, including Scripps Research’s Eric Topol, calling for an IN equivalent of the Operation Warp Speed (OWS) which originally produced the IM vaccines that have been in use in Europe and North America since late 2020. The hope is that an approved IN vaccine in the West may counteract the continued spread of the SARS-CoV-2 virus amidst waning efficacy of the IM vaccines against new virus variants.
The Long Haul
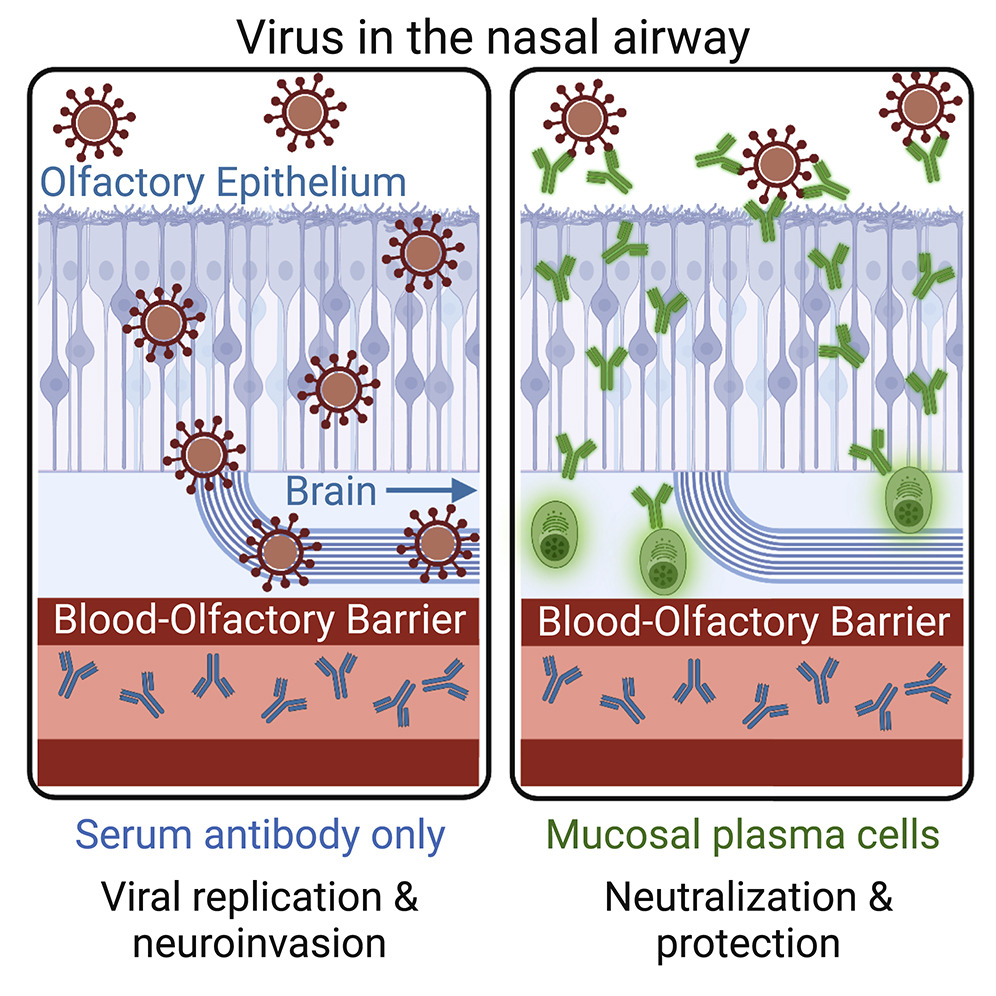 Viral infection with and without nasal mucosal immunity. (Credit: Wellford et al., 2022)
Viral infection with and without nasal mucosal immunity. (Credit: Wellford et al., 2022)An aspect of the SARS-CoV-2 virus that is becoming ever more pertinent is the collection of chronic conditions referred to as ‘Long COVID’, which includes blood clots (Knight et al., 2022) and negative neurologic outcomes (Xu et al., 2022). Notable with such Long COVID cases is that it was not necessary for the patient to exhibit severe COVID-19 symptoms, nor to have been hospitalized.
The reason for this is likely that although the IM vaccines induce an immune response in the vascular system which often efficiently protects the body’s organs, this does not seem to provide protection for the olfactory epithelium, nor the brain, both of which can be infected directly from the mucosal tissues of the nasal passages (Wellford et al., 2022).
Although an infection with SARS-CoV-2 provides convalescent immunity (i.e. from fighting off an infection) within the mucosal tissues, this immunity fades over time, much like the immunity provided by SARS-CoV-2 vaccination. Since each infection comes with the risk of permanent damage (and death), the ideal way forward would seem to be to have an IN booster twice a year (matching the ~6 month fall-off in efficacy), that may provide sterilizing immunity.
Essentially this is why IN vaccines are increasingly being looked at as a possible way to effectively deal with such respiratory viruses, as they should provide much better protection for the individual, while also limiting community spread.
Making IN Vaccines Work
Despite what one may think with already three IN vaccines in use with (emergency) authorization, IN vaccines are not very common. Perhaps the most well-known attempt dates from before the SARS-CoV-2 pandemic, in the form of the FluMist vaccine (LAIV) which to this date is the only FDA-approved IN vaccine. This flu vaccine is notable for using attenuated influenza virus, rather than the inactivated virus of IM flu vaccines, and provides efficacy comparable to IM flu vaccines. Its main attractiveness is that it avoids the use of needles, and does not require trained personnel to administer the vaccine.
What is challenging with testing IN vaccines is the lack of standardized tests for mucosal immunity. This is largely due to IN not having received much attention, which makes running large-scale trials of such vaccines and assessing their efficacy largely unexplored territory for many regulators. Even so, AstraZeneca and other pharmaceutical companies are currently running trials for IN SARS-CoV-2 vaccines.
Whether or not an IM vaccine can be adapted to work as an IN vaccine mostly depends on the type. The sub-unit type of vaccine (e.g. Razi Cov Pars) likely requires an adjuvant in order to create a strong enough response, while adenovirus-based IM vaccines can basically be used as-is, since as noted earlier, adenoviruses naturally infect mucosal tissue. For e.g. the AstraZeneca IN vaccine trials that are currently ongoing, the challenge would seem to be mostly in defining the efficacy, in the absence of clear protocols and techniques.
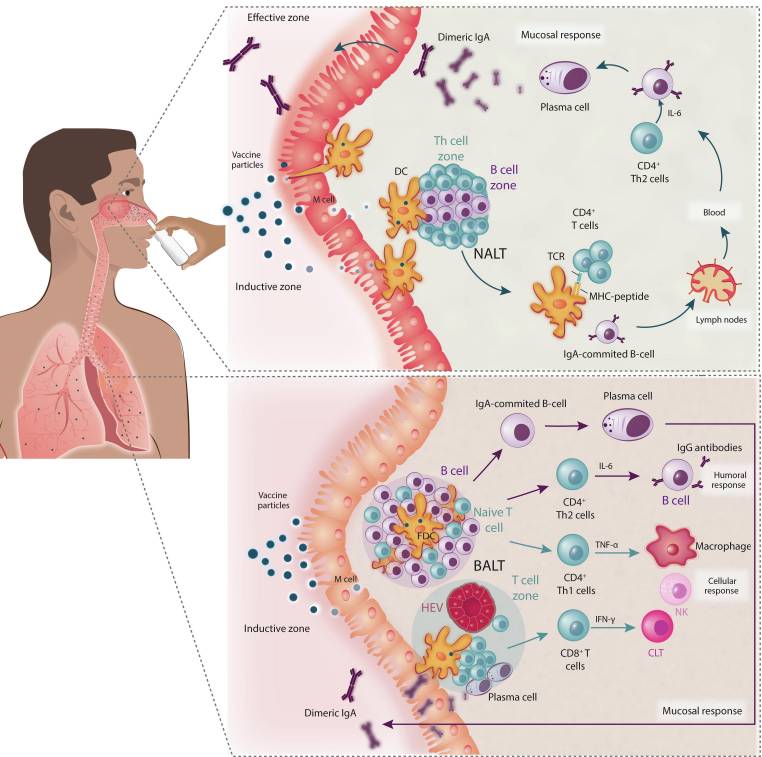 Effect of nasal vaccines on the upper and lower respiratory tract for the generation of mucosal and systemic immunity. (a) Protective immune responses in the nasopharynx-associated lymphoid tissue (NALT), with the pathogen-mediated reaction resulting mainly from by secretory IgA antibodies generated by mucosal epithelial cells. (b) Humoral immune response in the lower respiratory tract with bronchus-associated lymphoid tissue (BALT) having humoral as well as mucosal/local immune responses. Abbreviations: CTL, cytotoxic T lymphocyte; DC, dendritic cell; NK, natural killer; TCR, T cell receptor. (Credit: Chavda et al. 2021)
Effect of nasal vaccines on the upper and lower respiratory tract for the generation of mucosal and systemic immunity. (a) Protective immune responses in the nasopharynx-associated lymphoid tissue (NALT), with the pathogen-mediated reaction resulting mainly from by secretory IgA antibodies generated by mucosal epithelial cells. (b) Humoral immune response in the lower respiratory tract with bronchus-associated lymphoid tissue (BALT) having humoral as well as mucosal/local immune responses. Abbreviations: CTL, cytotoxic T lymphocyte; DC, dendritic cell; NK, natural killer; TCR, T cell receptor. (Credit: Chavda et al. 2021)Another challenge with IN vaccines is that the nasal mucosal surface provides innate protection against infections by forming a sticky trap that captures potential pathogens (Chavda et al., 2021). This is also why mRNA-filled liquid nanoparticles as used in IM mRNA vaccines do not seem to be a good match for IN vaccines. As these rely on having the body’s cells produce the target antibody from the mRNA, the lack of an effective way to get the mRNA into cells is a major hurdle, something which viral vectors by their basic design do not have to deal with.
Wait And See
With potentially billions of people across the world now having access to IN SARS-CoV-2 vaccines, there is the hope that this may do for the SARS-CoV-2 pandemic what the OPV did for polio in the 1950s and 1960s. Depending on the efficacy of these authorized IN vaccines, some regions and perhaps even nations may find themselves able to declare an end to community spread within a few years, if not less.
Meanwhile, Western pharmacological companies are still running their own IN vaccine trials that may deliver positive results by next year. All of which means that in the absence of an OWS-like push, Iran, India and China may provide us with the first glimpses of what a future with IN vaccines against respiratory viruses could look like as early as next year.
With some luck it may not only offer that much sought after off-ramp for the SARS-CoV-2 pandemic, but also provide IN vaccines with a much needed R&D boost. Who after all wouldn’t want a twice-yearly nasal spray that protects against even the common cold, or a more effective IN influenza vaccine?
Headline image: Untitled by Lauren Bishop for the Centers for Disease Control and Prevention
